
Brachial plexus injuries
Brachial plexus injuries result in the paralysis of the upper limb. These are generally serious and devastating injuries.
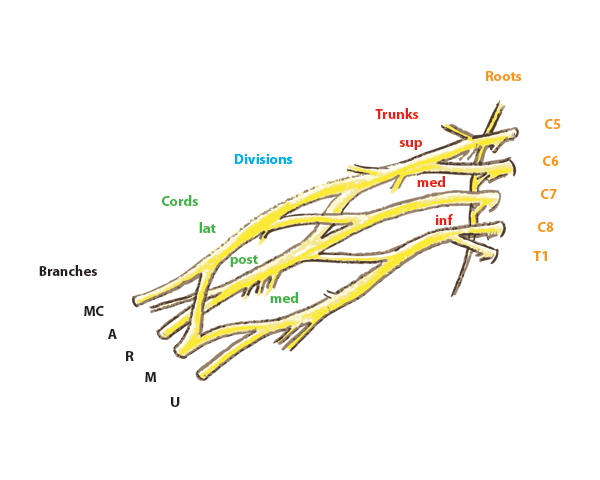
The injury involves the Brachial Plexus (Figure 1)
The brachial plexus consists of the nerve roots C5-T1 originating form the spinal cord.
Paralysis of the limbs can be reversible and non-reversible. Stopping blood supply to the nerves of the upper limb ( i.e. while lying on your arm when in a deep slumber) can cause temporary paralysis. However most injuries are sustained from falls and road traffic accidents in adults. When in occurs in newborns, termed Birth Brachial plexus injury, it is secondary to injuries sustained at the time of birth.
Non reversible injuries occur when the nerves that make up the Brachial plexus are either pulled from the spinal cord (avulsed) or the nerves break(ruptured) . This results in no connection between the spinal cord and the end muscle and skin resulting in loss of power and sensation. This is termed a flaccid paralysis. The area where there is a paralysis corresponds to the nerve roots that are injured and involved.
There can be some recovery in the paralysis over time if the injury is not too serious.
It is generally taken that if no significant recovery occurs by 3 months of the injury, there will be likely to have poor outcomes.